

Research vaccine communication
Research vaccine communication
We're overdue to re-focus to the long-term

Imagine a technology that, over the last 250 years, has prevented more premature deaths than any other health intervention. A technology that disproportionately saves childrens' lives. A popular and widely adopted technology.
Well, we have two out of the three.
Vaccines are suspected, rejected, and lied about daily. While much of vaccine research is a remarkable success - vaccine technologies have evolved to be safer and more effective - our communication has remained largely the same. It’s time for that to change.

Vaccine hesitancy is a tale as old as vaccines

When the first smallpox vaccine was available, there was significant concern and hesitancy. And wow does that make sense: it was a new technology (1) and it would make you sick. While the benefits were obvious the unknowns were scary and there was a sense of potential risk that was impossible to quantify.
Do you take your chances with the incredibly deadly smallpox, or do you try a technology that may have unknown consequences later? This question was especially difficult for parents - children are more likely to die from smallpox than adults (2), yet parents feared unknown consequences of the new technology.

The poliovirus was the same. Like smallpox, the poliovirus affects children more than adults, so parents were again in the hot seat when the polio vaccine became available. The risk of permanent paralysis and death from poliovirus is not insignificant. When the vaccine became available parents again hesitated and it took years to reach sufficient levels of vaccination to stop the spread of the disease in the United States.
COVID-19: new virus, same questions
Today we have a new pandemic with new characteristics, and a new vaccine to match. But the vaccine story is the same. Our initial response is the same hesitancy, with the same heightened hesitancy amongst parents on behalf of their children. To be clear, increased hesitancy from parents is 100% rational. It's the natural role of parents.

Each time a new vaccine comes out it faces hesitancy as though it's a completely new technology. But why? Most technologies see increases and accumulation in adoption over time - if you already own a computer the odds of purchasing a computer in the future is extremely high - and much higher than if you've never owned a computer.
The usual course of technology adoption
The first famously mass-produced car was the Model T. The Model T had a sidevalve, reverse-flow cylinder head inline 4-cylinder engine that primarily operated on gasoline. Engine technology has come a VERY long way since then. But here's the deal, if you look at motor vehicle adoption, it's not impacted by the changes in engine technology, safety technology, or any other change in vehicular design.
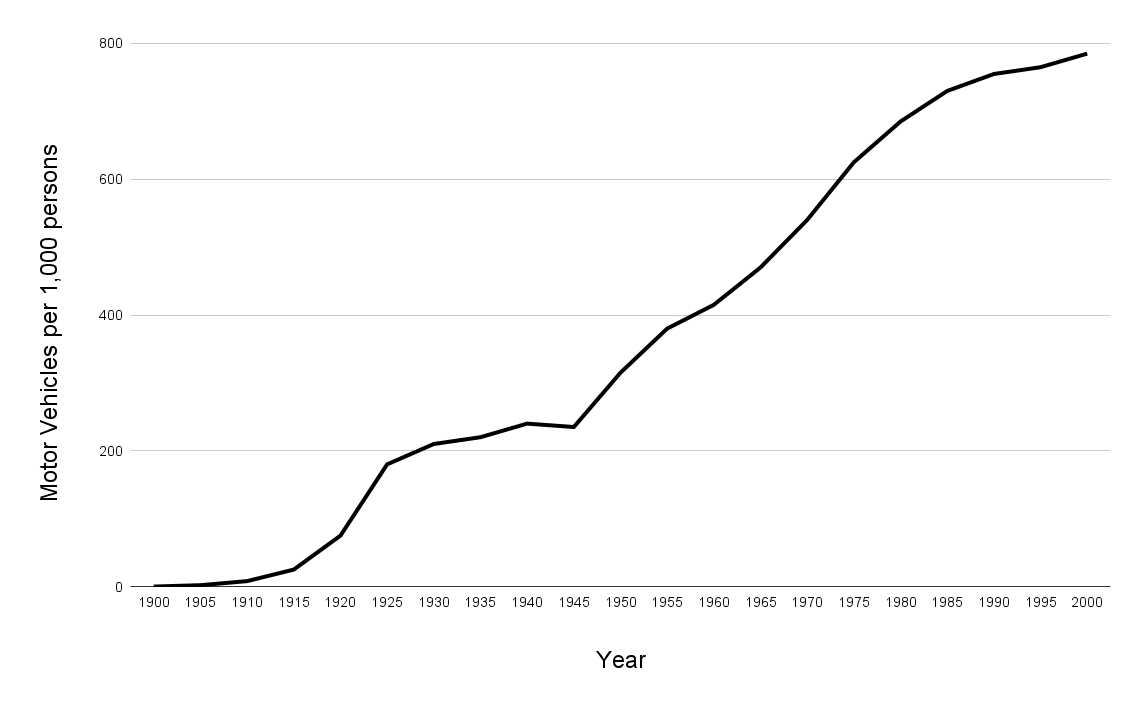
Over time, the benefits of automobiles has become increasingly evident to consumers, and adoption accumulated accordingly.
This general trend can be seen across technological innovations.
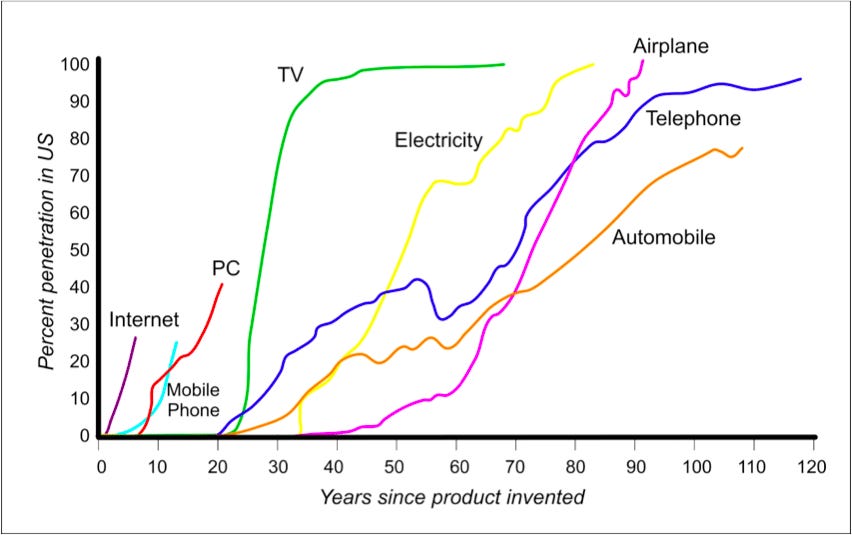
Generally speaking, technologies see accumulating adoption over time as the benefit is realized - despite the inevitable consequences of each technology. There are very few people who refuse to buy or ride in a motor vehicle because of the risk of car accidents, despite the fact that 38,000 people in the US die in accidents every year.
Tech adoption in healthcare
One hypothesis for why it's different in healthcare is because there is less perceived choice. You don't really opt-in to try a new healthcare intervention so much as you're stuck with your back against the wall choosing the least-bad option for getting out of a scary situation.
This almost certainly impacts enthusiasm, but across healthcare it doesn't limit adoption. For example, antibiotics. Antibiotics have significant side effects, but they also save lives and limit damage from bacterial infections. Unlike vaccines, antibiotics have been embraced too much: the overuse of antibiotics has created multi-drug resistant bacteria, most famously MRSA.
Vaccines face a tangibility problem
When you are symptomatic, interventions that reduce your symptoms are highly desirable. It's easy to appreciate the effect of an intervention when you literally feel it. Antibiotics have the obvious impact of resolving infections, just like Tylenol results in less pain. The benefit is obvious to the end-user.
Vaccines decrease the risk of a given disease. It's hard to tangibly appreciate that you didn't get sick when you never expected to be sick in the first place.
But just because something is hard doesn't mean that it's impossible. As President Kennedy once famously said in regards to going to the Moon, "...not because they are easy, but because they are hard, because that goal will serve to organize and measure the best of our energies and skills, because that challenge is one that we are willing to accept, one we are unwilling to postpone, and one which we intend to win, and the others, too.”
(quote is at 9:13, though the entire 18-minute speech is worth a listen)
When you ask the wrong question, you get the wrong answer

I'm not the first to notice that there is resistance to vaccines, and decades of research precede even my own conception. But here's the thing about research: you only get answers to the questions you ask. When it comes to communicating vaccines, and bio-as-tech in general, science has been asking the wrong questions.
Specifically, we've studied over and over how to maximize vaccine uptake in the short term. We've found answers to the question of how to get someone to take a specific vaccine on a specific day. We have not asked how to communicate vaccines in a way that is durable over time. We haven't asked what happens 6 months later when it's time for a different vaccine.
Short-term vs long-term
I get it, this sounds esoteric, but stay with me. Imagine you're in an area with a lot of tourism and you're walking through the shops. The vendors in this context are largely only concerned with whether you buy from them that day. As a result, you face a lot of aggressive sales tactics and coercive techniques. You may end up buying something, but the high-pressure approach has you avoid that part of town and those shops in the future. The short term outcome was a sale, but the long term outcome was avoidance.

In the world of vaccine communication research, the outcomes have focused on the short term: did you get that vaccine on that day. From this perspective, it's no surprise that one of the only consistently effective techniques found in studies is pretty aggressive and coercive: presumptive language. Presumptive language is basically when you assume a shared conclusion. "Now we're going to walk to the cash register and get you checked out." "Now we're going to get this shot."
Of course this is fine when everyone actually is in agreement. But if there's disagreement it creates layers of problems. False assumptions drive distrust, people feel coerced, and if questions are raised at this stage it catapults the conversation into one of dispute instead of collaborative discussion.
Different outcomes require different approaches
For the last 150 years we've seen the same response to vaccines, over and over again. The detailed reasons for concern trend differently over time, but the fundamentals remain the same.
And yet we continue to use the same bad approaches and the same flawed research design. We have to take a different approach, starting with admitting that we've been doing it wrong. It doesn't matter if someone gets a vaccine on a given day. It really doesn't - that's short-sighted.
It matters that people have trusted access to reliable information and that information has to be complete. It matters that people have an understanding of the value and opportunity that vaccines represent. It matters that people understand the risks of vaccines as well as the risks of the diseases the vaccines prevent. It matters that a person's concerns are openly discussed. Most of all, it matters that people are treated with respect throughout this process.
Trash the coercion, trash the judgment. Focus on the care in healthcare.
The concept of inoculation (giving a tiny amount of an infectious disease so that the immune system can learn to fight it without full-blown disease) emerged in Asia about a thousand years ago. The breakthrough attributed to Edward Jenner is the discovery that we could do this much more safely if the agent used for inoculation was a bit different. In the case of the original smallpox vaccine, he used cowpox as a way to generate an immune response in humans without full-blown disease. That's actually where we get the word vaccine - the latin term for cow is vacca. A good summary is here.
The death rate of smallpox for adults was 5-10%, whereas it could exceed 70% for children.
https://www.kff.org/coronavirus-covid-19/poll-finding/kff-covid-19-vaccine-monitor-april-2021/
https://www.researchgate.net/publication/264967305_The_high_cost_of_free_parking
Communicating vaccines among trusted health and social services providers is key to infectious disease management in developed countries, for sure. Tho initial population hesitancy seems persistent, there's reason to believe that this time, in the US, something else is happening among the covid vax-hesitant: historic socio-political polarization and deep institutional mistrust are taking a toll.
Some of that mistrust - especially among racial and ethnic minorities - is justified (think, Tuskegee, and current discriminatory access to care). Justified or not, Docs and other Providers - and the social service infrastructure that refers to them - must engage with communities who bear the inequitable brunt of this preventable bug and practice Population Health.
In addition to the evidence coming out (from Yale) about persuasive individual-level communications, Med Providers must lead in collective approaches (ads, psa's community events) and appeals to do our part to care for our communities.
This is a challenging shift for some Providers, steeped as they are in individual interventions (and rightly so). Pandemics require excellence there... and also transcending that frame by speaking to communities directly, and honoring the values that hold them together.
Lives depend on it urgently, as does every Doctor's ability to stay relevant now as a Preventionist.